This patient is a 38 yo office worker who was playing catch with her kids when she fell injuring her non-dominant left wrist. She was treated by a local orthopedist for 2 months in a cast. Due to continued pain she sought a second opinion. On presentation, she had very limited, highly nonfunctional, and painful wrist motion with tenderness over the thumb side (radial) of the wrist.
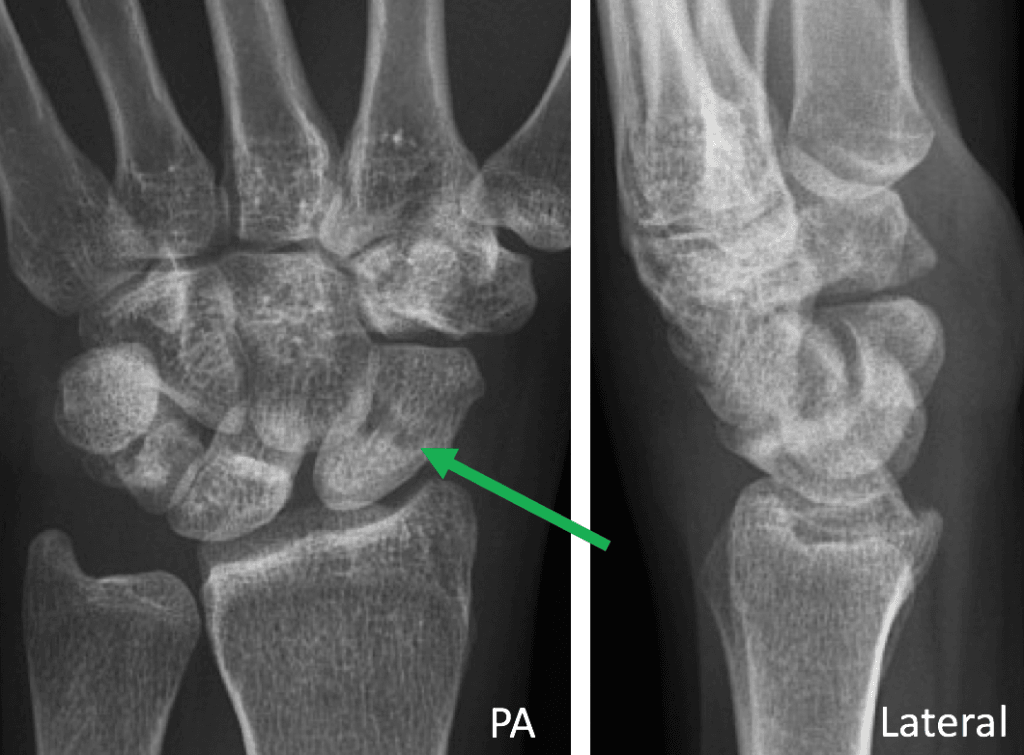
PA and lateral x-rays at presentation 2 months after the injury revealed a nonunited and angulated scaphoid waist fracture (green arrow) with resulting severe carpal instability as noted by dorsal tilting of the lunate on the lateral view.
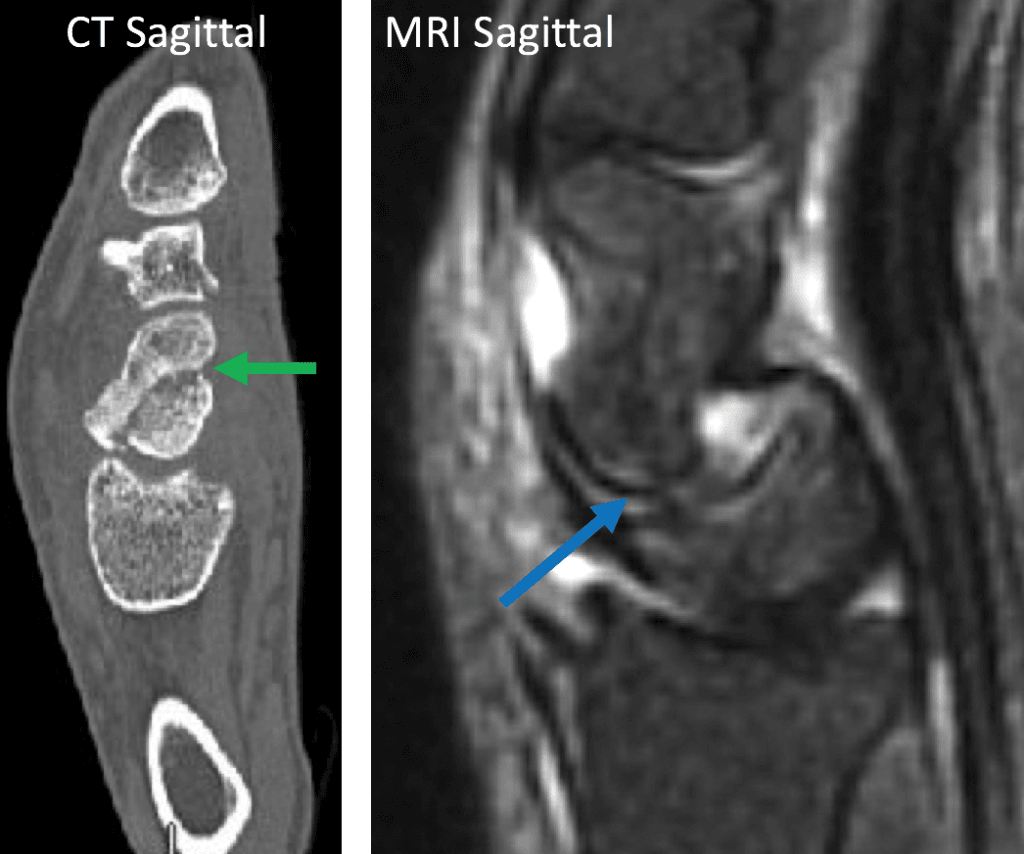
The CT sagittal image revealed the nonunion (green arrow) with fragment displacement and angulation that caused the carpal instability seen on the lateral x-ray. The MRI sagittal image demonstrated the degree of carpal instability between the lunate and the capitate which had caused early arthritic change. This sequence was the cause of the patients limited motion and pain.
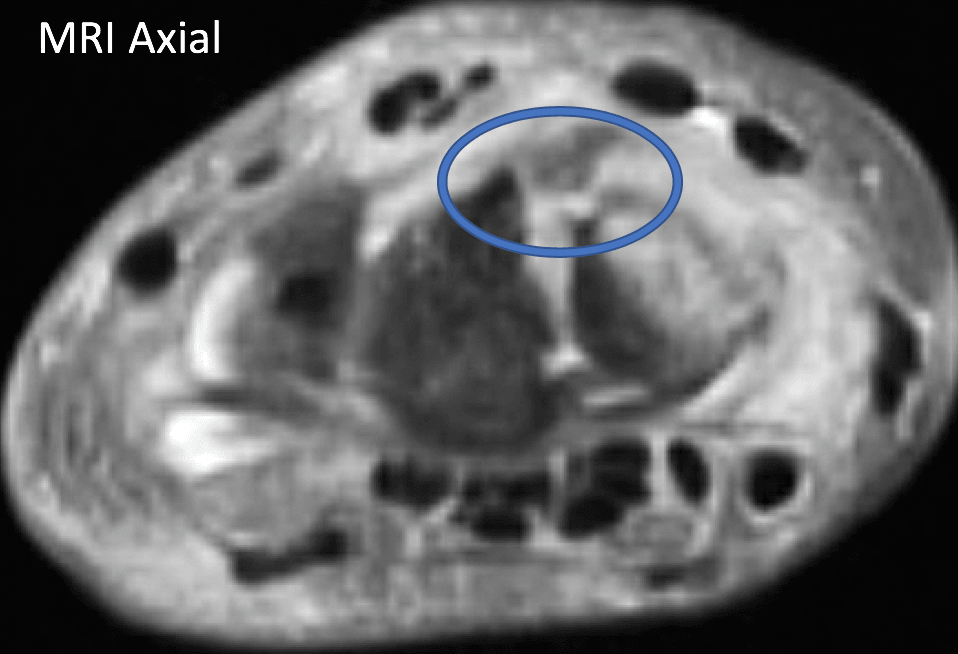
This axial MRI image seemed to indicate injury to the dorsal scapholunate ligament, potentially contributing, along with the fracture displacement, to the significant carpal instability pattern.
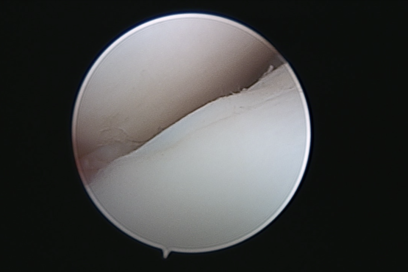
At surgery, arthroscopy was performed first in order to assure integrity of the scapholunate ligament using a minimally invasive technique. With the arthroscope in the dorsal 3-4 portal, the ligament was fully evaluated. This video shows completely intact fibers but with some evidence (hematoma) for injury dorsally, consistent with the MRI findings. This did not require ligament repair or reconstruction or additional incisions. I proceeded with surgery to repair the scaphoid bone.

In order to restore scaphoid anatomy, and correct the secondary carpal instability, a large bone graft (approximately half the size of the scaphoid) was taken from the iliac crest (hip), inserted into the prepared nonunion site, then stabilized with one intramedullary, buried compression screw. The patient was immobilized in a cast for 6 weeks then began therapy with a removable splint.
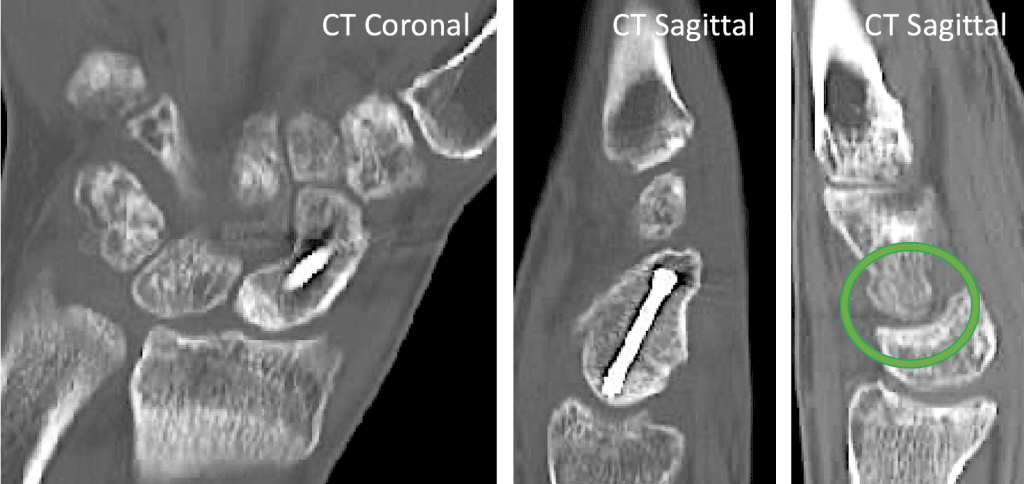
The CT images 3 mos after surgery revealed that the nonunited scaphoid had healed and the carpal instability (position of the lunate relative to the capitate) was corrected (green circle). The patient regained painless motion and excellent function.

High impact professional athlete with wrist pain affecting function and performance. His subtle MRI findings…
Professional golfer with persistent pain over the small finger side (ulnar-sided) of his wrist preventing…

This is a professional basketball player who fell on the court and had immediate wrist…
{kind=link}