This patient was a 52 yo male electrician with hand pain and clicking/locking noted with flexion of his middle and ring fingers. He was diagnosed with “trigger finger” and cortisone injections were attempted in the office. They alleviated his symptoms temporarily, but not completely. For that reason we performed trigger finger releases. At the time of surgery, after the standard release of his ring and long finger A-1 pulleys was complete, he was asked to actively flex and extend the operated fingers. Despite a full pulley release, the long finger continued to click and catch. For that reason, a resection of the ulnar slip of his flexor digitorum superficialis (FDS) tendon to that finger was performed, eliminating the catching. Therapy was initiated early and he regained painless motion of all fingers.

The first approach to treating a “trigger finger” is usually a cortisone injection. This is done in the office after freezing the skin. A fine needle is used to inject a combination of 1% lidocaine and betamethasone into the flexor tendon sheath in the region of the A-1 pulley (shown). In a successful injection, the patient typically feels the medication travel up their finger as the cortisone fills the tendon sheath. The finger may remain numb for an hour or so after the procedure and then in some individuals might be a bit more sensitive for a day or so. After that has resolved, the pain begins to go away, but often the clicking takes several weeks to abate. Significant loss of motion or recurrence after a successful injection are indications for surgery.
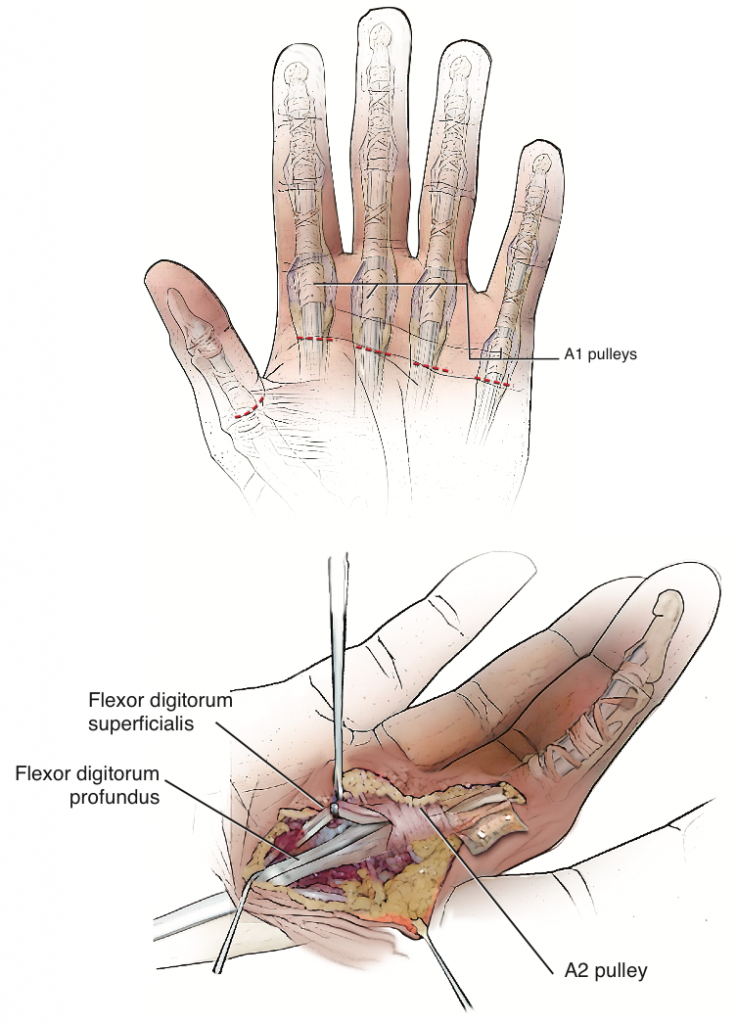
The surgical incision is made in line with the involved finger, often in a skin crease. In this patient’s case, two small 6mm incisions were made to release the A-1 pulleys of each finger. This simple release was not enough for the long finger and as a result it was extended another 4mm (less than that shown on the drawing). You can see on the drawing that each finger has two flexor tendons, the flexor digitorum profundus (FDP) and the flexor digitorum superficialis (FDS). Both must travel back and forth under the pulley system. Here the A-1 pulley has been cut and the A-2 pulley is visible.
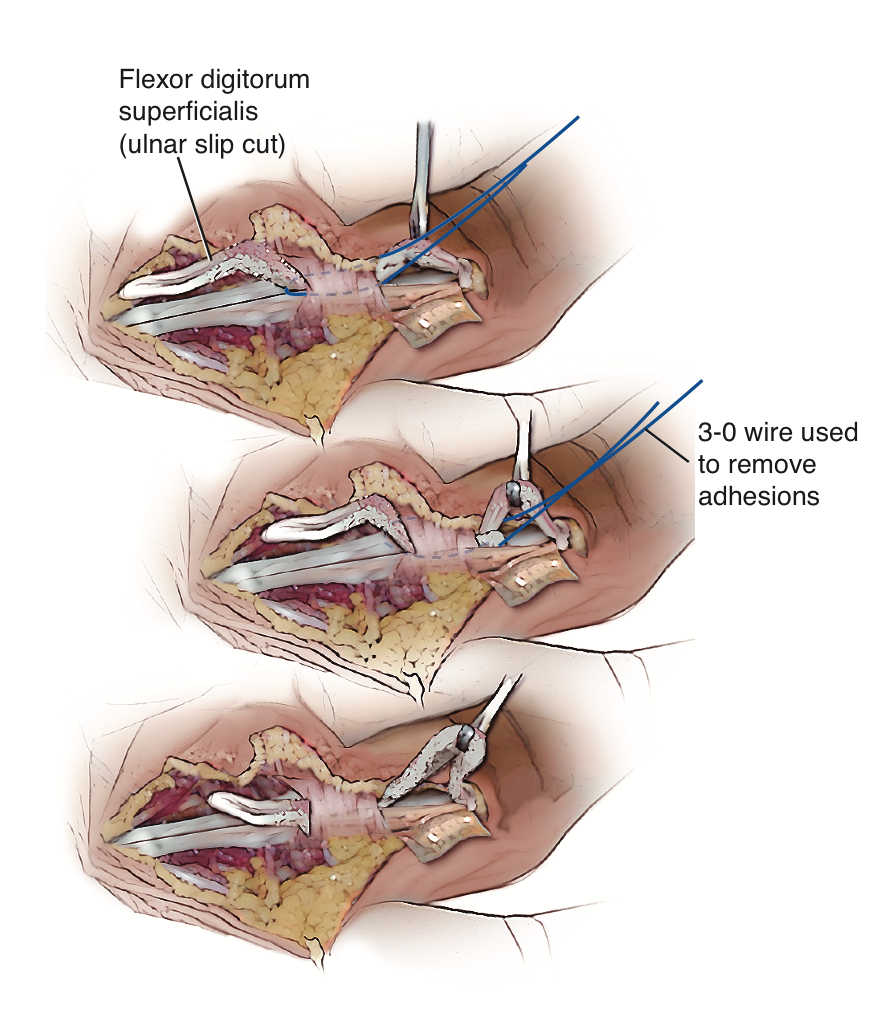
Given that additional pulleys cannot be released without risking finger function, a portion of the FDS tendon (the least important of the two) was removed to make space within the flexor canal and eliminate the catching. This form of treatment over and above an A-1 pulley release is required in only a very small percentage of patients but is most common in diabetics.

High impact professional athlete with wrist pain affecting function and performance. His subtle MRI findings…
Professional golfer with persistent pain over the small finger side (ulnar-sided) of his wrist preventing…

This is a professional basketball player who fell on the court and had immediate wrist…
{kind=link}