This patient is a 20 yo right hand dominant Division 1 college defensive back who became a perennial starting NFL player. During a game, he fell on his left wrist defending a pass. He landed on the palm, just below the thumb, sustaining an extension and supination (palm up) force. Though he had immediate pain, he continued to play protected for another 4 months. After the season, he presented for treatment

The PA x-ray reveals a triquetral fracture (green arrow), signifying a more global wrist injury, likely involving the intercarpal ligaments, including the scapholunate ligament (holds the scaphoid and the lunate together). On the PA and lateral x-rays the relationships of the carpal bones, including the scaphoid (S) and lunate (L) are correct. There is no “static” instability within the wrist
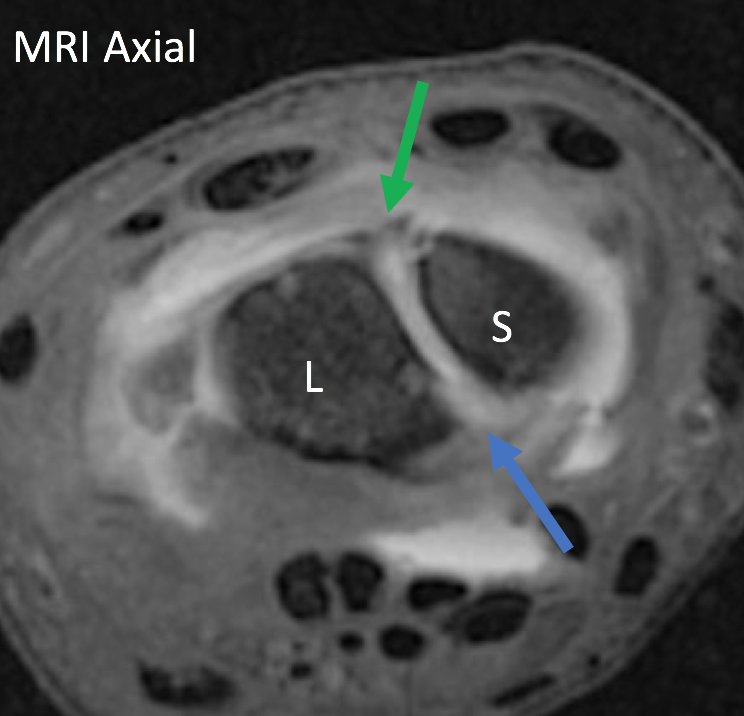
This axial MRI image depicts the scapholunate joint (S = scaphoid & L = lunate). The green arrow is highlighting the injured dorsal portion of the scapholunate ligament on the back of the wrist, the critical stabilizing component, and the blue arrow points to the injured volar component.
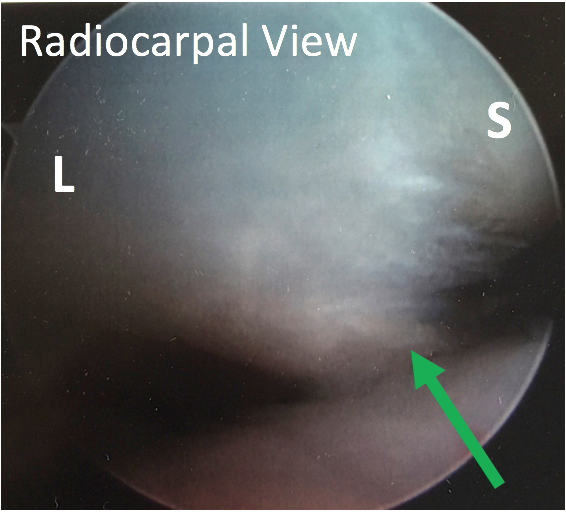
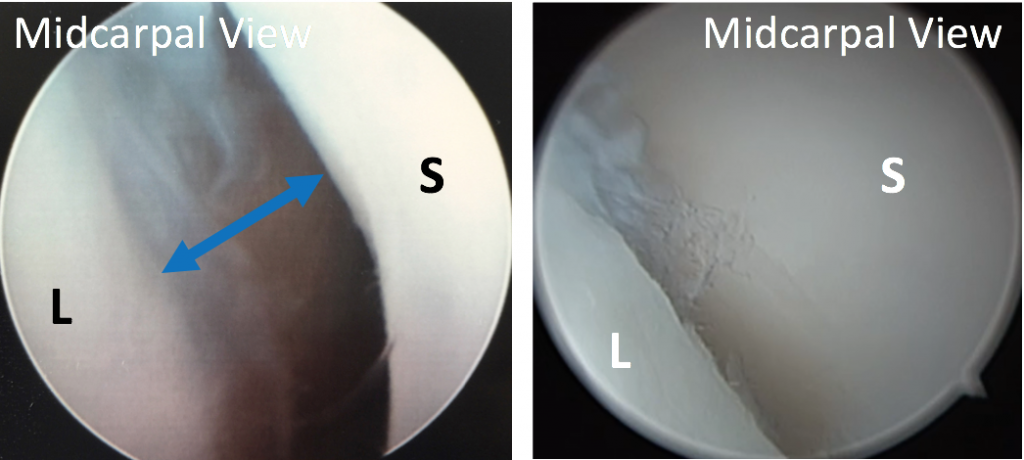
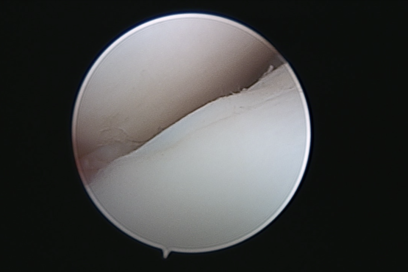
Prior to making an open incision and repairing the ligament, the degree of injury was better defined in a minimally invasive way using arthroscopy. Looking from the back of the wrist you can see the torn scapholunate ligament underneath the scapholunate joint (radiocarpal view) and the instability resulting from the tear above the joint (midcarpal view – picture and video). S = scaphoid L = lunate
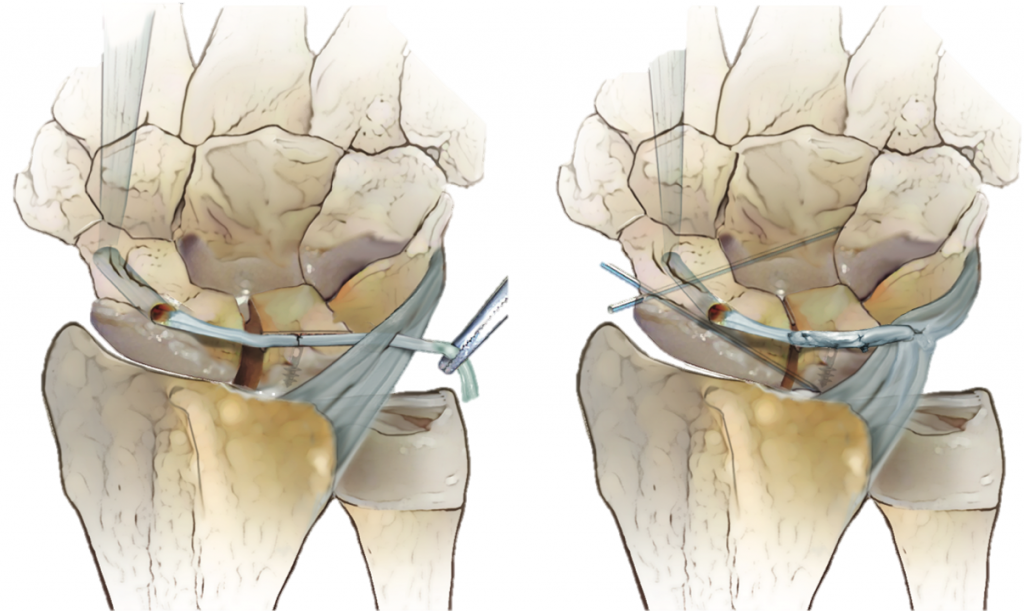
Given the degree of instability noted arthroscopically and the chronicity of the injury, a modified Brunelli tenodesis was performed. The flexor carpi radialis tendon was brought from the palm side to the back of the wrist through a bone tunnel drilled in the scaphoid and then used to reconstruct the scapholunate ligament.

The bones are pinned in place for approximately 10 weeks after surgery to allow the reconstruction to heal. The 4 pins are then removed and therapy is initiated. Full use is not allowed until 4-6 months after surgery
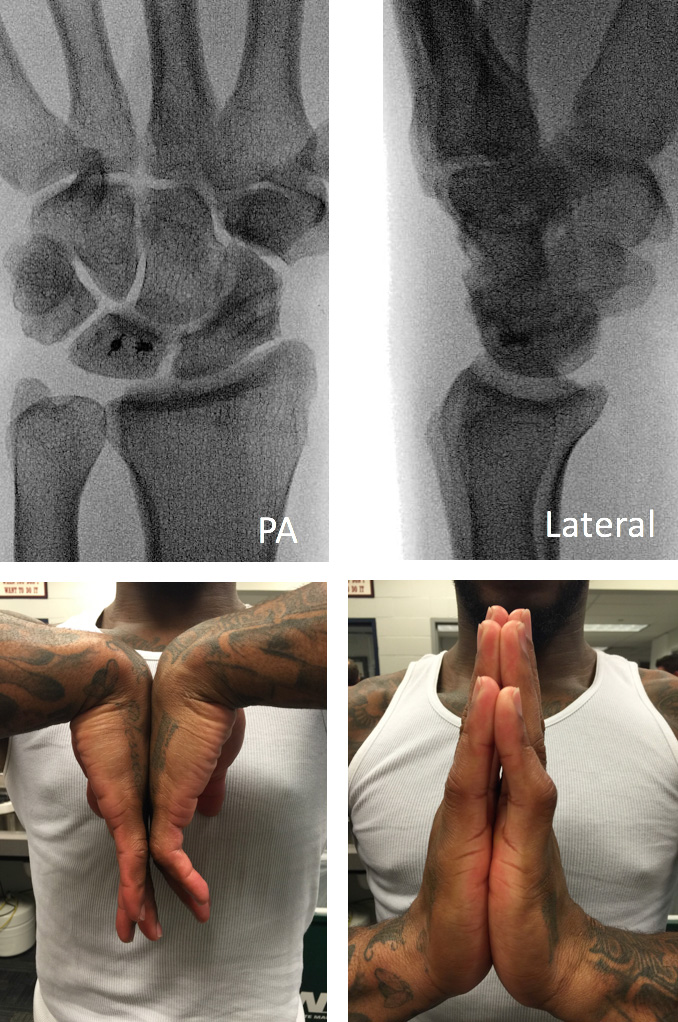
Eight years after surgery, this player is still starting in the NFL without complaints of pain or stiffness. Though he did regain full wrist motion, a byproduct of this stabilization procedure is usually stiffness with some loss of flexion > extension.

High impact professional athlete with wrist pain affecting function and performance. His subtle MRI findings…
Professional golfer with persistent pain over the small finger side (ulnar-sided) of his wrist preventing…

This is a professional basketball player who fell on the court and had immediate wrist…
{kind=link}